If you’re considering full-arch dental reconstruction — commonly advertised as “All-on-4” or “All-on-6” — congratulations: you’re looking at some of the most predictable, life-changing solutions modern implant dentistry offers. This guide walks you through the technical differences, when clinicians tend to prefer one over the other, realistic cost ranges in popular medical-tourism destinations, what to expect from longevity and maintenance, and practical tips for choosing a clinic abroad. I’ve pulled together clinical evidence, long-term outcome studies, and real-world cost data so you can compare options confidently and make a travel plan that balances safety, quality, and value.
What are All-on-4 and All-on-6?
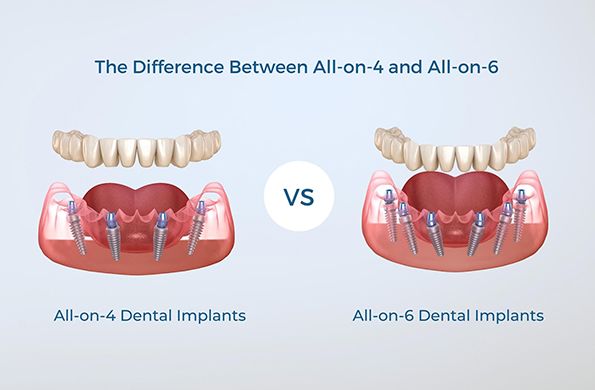
Both All-on-4 and All-on-6 are concepts for immediate-loading, full-arch fixed prostheses supported by dental implants. Instead of placing an implant for every missing tooth, a complete arch (upper or lower) is supported by a small number of implants onto which a fixed bridge is attached. The key difference is the number of implants used:
-
All-on-4 — four implants per arch. Often two anterior implants are placed vertically and two posterior implants are tilted to maximize bone contact and avoid sinuses or nerve canals.
-
All-on-6 — six implants per arch. Implants are usually placed more evenly across the arch and typically all vertically oriented (but variations exist).
Both approaches may use immediate provisional (same-day) teeth, followed by a definitive prosthesis after healing. The goal is to restore chewing function and aesthetics with a fixed, non-removable solution.
Clinical differences in simple terms
-
Support distribution: Six implants spread biting forces over more fixtures and more bone area. Four implants concentrate forces on fewer anchors, which can increase mechanical demands on each implant and the connecting prosthesis.
-
Surgical complexity: All-on-4 can often be performed with less grafting because tilted posterior implants avoid anatomical limitations. All-on-6 sometimes requires more bone volume or grafting to get six good implant sites.
-
Cost and time: More implants mean higher surgical and hardware costs and sometimes longer chair time. All-on-4 is often marketed as a lower-cost, faster option.
-
Prosthetic maintenance: With fewer implants, prosthesis maintenance (e.g., screw loosening, framework fatigue) can be slightly more frequent but still uncommon when done well.
In practical clinical studies, the survival rates and short- to medium-term outcomes for four vs six implants are very similar in well-selected patients. Several comparative analyses and randomized trials have found no clinically meaningful difference in implant survival or prosthetic success between All-on-4 and All-on-6 at 2- to 5-year follow-up points, although All-on-6 can show small advantages in certain radiographic measures and perceived predictability by some clinicians.
When clinicians prefer All-on-4
All-on-4 is often chosen when:
-
The patient has significant posterior bone resorption and the tilted posterior implants avoid sinus lifts or heavy grafting.
-
Cost or treatment time is a major constraint and the patient wants the least invasive option that still delivers a fixed arch.
-
Immediate loading (same-day teeth) is a priority — All-on-4 workflows were popularized specifically to enable immediate provisional prostheses with fewer implants.
-
The patient’s occlusal scheme and parafunctional habits are manageable, and a clear, experienced surgical/prosthetic team is available.
When clinicians prefer All-on-6
All-on-6 is commonly favored when:
-
There is enough bone for six implants without complex grafting, and the clinician wants to maximize load distribution.
-
The patient has strong bite forces, bruxism, or other risk factors where additional implants provide a mechanical safety margin.
-
The clinician or restorative team prefers more anchor points for future repairs, hygiene access, or staged protocols.
-
The treatment plan allows for slightly higher cost and more surgical time in exchange for potentially increased redundancy.
One pragmatic point from clinical surveys and trials: more experienced implant teams and prosthodontists sometimes favor All-on-6 for predictability in certain clinical situations, while All-on-4 remains perfectly valid when indications fit.
Outcomes and longevity — what the evidence says
A growing body of evidence supports excellent medium- and long-term outcomes for immediate full-arch protocols. Large longitudinal studies following patients for a decade or more report high prosthetic survival (many studies >95% prosthetic survival across years) and implant survival rates often in the 90–95% range at long-term follow-up. One long-term cohort study that followed patients for 10–18 years reported cumulative prosthetic survival near 98.8% and implant survival around the low-to-mid 90s percentage, with modest marginal bone loss over time — outcomes that are reassuring for patients committed to long-term care.
Comparative papers looking specifically at 4 vs 6 implants in immediate full-arch restorations found no significant difference in survival rates at 2–5 years — both protocols perform extremely well when executed correctly. Some studies note slightly better radiographic or biomechanical metrics with six implants in specific scenarios, but these differences rarely translate to clinically meaningful failure rates in routine practice.
Key takeaway: With modern implant systems, careful case selection, and experienced teams, both All-on-4 and All-on-6 offer durable, functional results that can last a decade or longer — provided good oral hygiene and regular maintenance.
Expected costs (medical-tourism perspective)
Costs vary widely by country, clinic, implant brand, materials (acrylic vs. hybrid vs. zirconia), and package inclusions (flight, hotel, transfers, scans, sedation). Below are realistic ranges you’ll see when shopping clinics abroad — use them as a planning benchmark, not a final quote.
-
Turkey (very popular for dental tourism): Many clinics advertise low headline prices for All-on-4; typical package offers range from roughly $2,500–$7,000 per arch for economy packages up to premium packages that are higher. Pricing depends heavily on the implant brand, prosthesis material, and included services. Turkey’s combination of cost and a mature dental tourism market makes it a common choice.
-
Hungary / Central Europe: Hungary is a European hub for dental tourists. Average reported ranges for All-on-4 or All-on-6 per arch tend to fall in the $5,000–$12,000 range depending on the clinic and materials. Hungary often balances European regulatory proximity with lower costs than Western Europe.
-
Mexico: Popular with North American patients, Mexico’s All-on-4 packages typically range from $6,000–$15,000 per arch depending on city, clinic, and package inclusions. Some border towns have lower prices; resort cities may charge more.
-
Other regions (Thailand, Poland, Spain, etc.): Prices and quality vary. Always check which implant systems are used and whether follow-up care is included.
Note on All-on-6 pricing: Expect All-on-6 to cost more than All-on-4 roughly in proportion to the additional implants and surgical time — typically an extra 20–40% depending on implants and lab work. Exact differences depend on whether the prosthetic framework and lab fees are priced per arch or per implant.
What’s included in most medical-tourism packages
A well-structured package should transparently list: pre-op CBCT scans, consultation, implant brand and number, provisional same-day prosthesis, final prosthesis (material: acrylic hybrid vs zirconia), anesthesia/sedation, medications, post-op checkups, and support for travel logistics. Some clinics include two trips (surgery and finalization) while others do both stages during one stay with local follow-up. Always confirm:
-
Implant brand and warranty / follow-up policy.
-
Clear timeline for temporary → final prosthesis.
-
If complications arise after you return home, who is responsible for management and cost?
-
Whether an international guarantee is in writing.
Risks, complications, and maintenance
Both All-on-4 and All-on-6 carry implant-related risks that are uncommon but real: infection, implant failure (early or late), prosthetic screw loosening, framework fracture, peri-implantitis, and bone loss. Most failures are manageable if detected early. Important practical points:
-
Hygiene and maintenance: Fixed full-arch prostheses require diligent hygiene — interproximal brushes, water flossers, and regular professional cleanings are essential. Neglect increases risk of peri-implant disease.
-
Bruxism and habits: Heavy grinders may require night guards or stronger frameworks (titanium-reinforced or zirconia) and sometimes prefer additional implants (All-on-6).
-
Follow-up care: Regular checkups (6–12 months) with radiographs help detect bone loss early.
-
Complications abroad: If you travel for treatment, ensure there is a clear plan for managing complications when you’re back home — this may require an agreement with your local dentist.
A final practical caution from public-health observers: low prices alone are not a reliable quality marker. Some health systems have reported increased presentations from patients with complications after low-cost overseas procedures; thorough vetting is essential.
How to choose between All-on-4 and All-on-6
There’s no one-size-fits-all answer. Ask your implant team to evaluate:
-
Bone volume and anatomy: Do you have enough bone for six implants, or would that need grafting? Tilted implants might avoid grafts.
-
Medical and dental risk factors: Smoking, diabetes, prior radiation, or periodontal disease can affect prognosis and may tilt the decision.
-
Functional demands: Heavy bite force or bruxism often favors more implants or reinforced prostheses.
-
Budget and logistics: If grafting or staged treatment is required for All-on-6, costs and travel increase.
-
Clinician experience: Choose the option the treating team has the most documented success with — surgeon skill and restorative planning matter more than the number of implants.
Many experienced teams will present a patient-specific plan showing why they recommend 4 vs 6 implants — that explanation and the evidence they provide is a good test of their professionalism.
Questions to ask a clinic (short checklist)
-
Which implant brand and prosthetic material will you use?
-
Can I see before/after cases and contactable patient references?
-
Is a CBCT included and will I get a digital treatment plan?
-
What is included in the price (scans, pre-op tests, sedation, temporary/final prosthesis, post-op visits)?
-
What is your complication policy and emergency contact after I return home?
-
Who will perform each part of the treatment (surgeon vs prosthodontist)?
-
Is there a written warranty and what does it cover?
Realistic expectations after surgery
-
Immediate appearance: You’ll usually leave the clinic with temporary fixed teeth the same day or within 24–48 hours.
-
Eating: Start with soft foods; full chewing resumes gradually as healing occurs. Avoid very hard or sticky foods initially.
-
Healing timeline: Soft tissue healing in weeks, osseointegration in 3–6 months for most cases; definitive prosthesis typically delivered after this healing period.
-
Longevity: Many patients enjoy a decade or more of reliable function with proper care; components may need maintenance or replacement over the years (e.g., acrylic versus zirconia teeth).
Final practical travel tips for medical tourists
-
Don’t book the cheapest flight + clinic package until you’ve verified credentials, patient reviews, and implant brand details.
-
Plan for at least one extra trip or a longer stay if complex grafting might be needed.
-
Bring a detailed written treatment plan and copies of medical records to your local dentist for continuity of care.
-
Budget for follow-up care at home — minor maintenance expenses are normal.
-
Consider travel insurance that covers medical procedures or complications, and check whether your home clinician is willing to take on post-op care if needed.
Bottom line
Both All-on-4 and All-on-6 are proven, effective solutions for full-arch restoration. Clinical evidence shows similar survival rates at medium-term follow-up for carefully selected cases, while long-term studies demonstrate strong prosthetic survival and good implant survival when procedures are performed by experienced teams. The difference between choosing four or six implants often comes down to anatomy, risk factors, clinician preference, and your willingness to accept additional cost and possible grafting. If you’re traveling for treatment, prioritize transparent pricing, a clear treatment plan, quality implant systems, and documented aftercare — value is about predictable outcomes, not just the lowest headline price.








